Report / Edited by: Roberta Kline, MD
3/18/2024‐ In a recent review on the latest medical diagnostic innovations in early detection and interventional imaging, MIT NEWS published a review on the development of the wearable breast ultrasound patch. This device is designed to be integrated into a bra for long term use, allowing for more frequent monitoring of patients at high risk for breast cancer from the convenience of their home. Dr. Tolga Ozmen, a breast cancer surgeon at Massachusetts General Hospital who is also an author of the study gave us an exclusive interview about the concepts behind this technology and his clinical involvement leading to bringing this groundbreaking diagnostic device to market.
Dr. Tolga Ozmen is a breast surgical oncologist affiliated with Mass General Hospital and is a faculty at Harvard Medical School. He highlights that the inventor of this novel wearable ultrasound device is Dr. Canan Dagdeviren and her team at the MIT Media Lab. Dr. Dagdeviren, known for her distinguished contributions to science, shares a common research interest with Dr. Ozmen which is advancing breast cancer detection and early diagnosis, which has brought their paths together.
<
INTERVIEW with Dr. Tolga Ozmen
As the study is still ongoing, I cannot discuss the full details‐ but I can tell you that our preliminary results were very successful. It was published in the Journal of Science Advances. Our wearable ultrasound device showed similar performance measurements as conventional ultrasound device in detecting breast lesions.
The results of our preliminary study are very compelling. In the next phase of our study, we will be exploring the performance of our device in a larger cohort of patients. Our objective is to confirm a baseline of (at least) the same performance as the conventional models – within a much larger number of patients. And if everything goes as planned, I don't see any reason why we can't hit the market in the next 10 years.
This device will contribute to breast imaging by offering a convenient method to screen women with dense breast tissue or women with high breast cancer risk. Our device is a wearable bra- shaped automated device that the patient will put on herself. The patient can do this easily and take this device home for their convenience. The images will be taken by the ultrasound patches placed on the cup‐shaped conformable device, and the data will be sent to a central unit via wifi.
 |
| Source: MIT News |
Deep learning based algorithms will generate the interpretation of these images and if any concerning findings are detected, it will alert us and the patient will be recalled to a radiology unit or a breast health center for additional imaging or an additional physical exam. For this reason it has the potential to be used as the first step for screening in patient with high risk or dense breast tissue. Today's breast cancer treatment is becoming more personalized as a result of increased knowledge. We can now tailor treatments to patient demographics ( i.e. race, age) and tumor characteristics. With accumulating knowledge, we can now also extend personalized approaches to screening strategies including modalities and frequency intervals based on each woman's breast cancer risk.
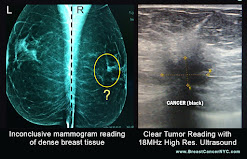
The current standard in breast cancer screening for average risk women includes yearly breast exams and mammograms starting at age 40. This is an effective screening method for decreasing breast cancer mortality in average risk population, backed by numerous published research studies. But we also know that mammography has been shown to be inferior to other imaging modalities in certain cases, including women with dense breast tissue. In the presence of moderate or extreme density of breast tissue, the sensitivity of mammogram decreases significantly, reducing the ability to detect breast cancer. In these women, supplemental imaging modalities in addition to mammography are often indicated.
In some cases, there are findings on the screening that require close follow up. Especially if these women are already identified as being at higher risk, they would benefit from follow up in 3-6 months rather than the standard one year.
I think our device is the perfect solution for these and other similar scenarios because it makes the follow-up surveillance much easier for the patient and the physician. Another benefit is that our device uses an ultrasound technology which is ideal for reading dense breast tissue. Ultrasound is very efficient and is highly sensitive for detecting abnormalities in dense breast tissue, and this is especially relevant for younger patients at high risk due i.e., inherited genetic mutation, etc.. These women can be screened with this device more frequently, and this device makes it easier because they can take it home and wear it regularly rather than having to take time to go to frequent imaging appointments. This paradigm has the potential to greatly improve accessibility and increase compliance with breast cancer screening.
We potentially see patients wearing this device as often as every couple of months, enabling us to detect changes early. There are often scenarios where screening mammography and/or ultrasound may show abnormalities that aren’t concerning enough to warrant biopsy but do benefit from close follow-up. Often the patient is requested to come back in 3-6 months. Wearing this device between mammogram visits could offer new data in the form of significant changes in the size or characteristics of that abnormality. Any new images can be generated and reviewed at the central unit, and compared with previous imaging. This interventional imaging allows us to watch the changes on a particular mass or lesion more closely and intervene sooner than their regular screening schedule when warranted.
INTEGRATING WEARABLE BREAST SCANNER WITH CURRENT IMAGING SCHEDULES
I envision that insurance companies, hospitals, or imaging centers would carry our device and lend it to patients who need frequent follow-ups. If the patient has increased risk or has suspicious lesions as I described, our device may be helpful in detecting any changes or abnormalities much earlier, and then these patients can be invited back to the hospital or breast imaging center for further workup. There is also a great benefit to the patient who feels less stressed knowing that she is receiving close attention, rather than worrying until her next scheduled imaging appointment.
AFFECTING PERSONALIZED TREATMENT WITH EARLY DETECTION
I want to emphasize that every woman has different rate of risk for breast cancer. This is why it is important to personalize each woman’s screening strategy. For average risk women, starting mammograms at age 40 is the standard recommendation, but we know that doesn’t fit many women who are at higher risk and may not even know it. We also recommend that women increase their awareness of breast cancer starting at a younger age, including knowing thE signs of breast cancer and how to do their own breast exams. It’s also important that if they have any concerning findings, symptoms, or signs, they also need to know to approach their primary care physician, gynecologist or a surgeon for an exam and to discuss their concerns and feel that they are taken seriously.
Breast cancer screening itself doesn't only include mammograms or other imaging. It also includes a patient's self‐awareness, and we recommend women start doing self breast exams by the age 20‐25 and knowing the signs, symptoms, and risk factors that increase (and decrease) breast cancer risk. This expansion of what is considered part of breast cancer screening is very important, and is why we're trying to do as much as we can in order to increase awareness.
Assessing a woman’s risk enables us to further personalize her strategies and screening schedule. High risk patients may have inherited gene mutations, a family history, or both. For these women we typically start screening them with a mammogram or MRI 10 years younger than the first family member with breast cancer. For younger women that start at age 20‐25, we typically will screen with an MRI until after age 30, when we may add mammography as per recommended guidelines.
Reference & Image Sources: https://news.mit.edu/2023/wearable‐ultrasound‐scanner‐breast‐cancer‐0728
A TRUE GAME-CHANGER IN BREAST TREATMENT MONITORING
"As Breast cancer continues to be the second leading cause of cancer death in women, the battle continues and one of our best weapons in this fight is the innovative use of technology. Screening and diagnostic protocols are a major part of imaging but so is image guidance and monitoring. This technology offers significant promise in the tracking and treatment support on a logistical level. The idea of a wearable imaging monitor gives both the patient and the physician better data as to treatment progress and/or potential malignancy. It uses remote/wifi technology in the best way- by connecting the patient directly to the central monitoring specialist in real-time, eliminating any delays and appointment waiting." -
Dr. Robert L. Bard -breast cancer radiologist, NYC
A major concern is the presence of breast cancer in underserved communities, including those TOO YOUNG FOR A MAMMOGRAM. Whereby the medical community touts the recommended (and legal/billable status) of getting a mammo scan should be between 40-50, what happens to the many women who do not fit this age criteria? How would they even know to get checked without the support of their clinicians or an alarm from family history? Decades into the battle against breast cancer, clinicians and the public are much more educated about EARLY DETECTION, PREVENTION and the current protocols and modalities available to save lives. Recent headlines on DENSE BREAST and the advancements in ULTRASOUND SCANNING supports a major part of this battle. SEE COMPLETE FEATURE
2022 REVIEW ON WOMEN'S EARLY DETECTION STANDARDS
Breast cancer is still one of the most common cancers in women, and the leading cause of cancer mortality. While mammography is considered the standard imaging for early detection, it falls short for many – including those with dense breasts. Approximately 40% of women have dense breasts, which we now know is associated with an increased risk of breast cancer. On top of this increased risk, mammogram is less sensitive for early detection – up to 50% less for women with the highest breast density. [1] As a result many women are not diagnosed until they have a much later stage cancer – and a worse prognosis. [2]
The State of Connecticut passed legislation requiring notification of breast density in 2009, after having passed legislation requiring insurance coverage for ultrasound for dense breasts in 2005. As an ObGyn physician practicing in CT at the time, I remember the discussions with colleagues and patients around this issue although at the time there were no formal efforts to raise awareness or update guidelines from our national specialty organization, the American College of Obstetricians and Gynecologists (ACOG).
PERSPECTIVE: PERSONAL FINDINGS BY A CLINICAL PROFESSIONALI was fortunate to have benefited personally from this effort when I had my first screening mammogram shortly after the law went into effect. The reading radiologist personally informed me of my high breast density immediately after the mammogram, and after recommending a breast ultrasound for further evaluation this was done right then and there. I walked away from my appointment feeling well informed, and any potential anxiety relieved by the prompt additional imaging and results. I also knew that I needed a different approach for my screenings going forward.
Between 2009 and 2019, 37 other states and D.C. passed legislation requiring notification of breast density, one of the last being my new home state of New Mexico. In 2019 a federal law was passed to require both clinician and patient reports contain plain language around the woman’s breast density, and to discuss with her provider. The FDA then created standard language that has now been implemented, requiring reporting on a woman’s individual breast density, and recommendation to discuss with her provider.
There is still much to be learned about what causes dense breasts and why women with dense breasts have an increased risk of breast cancer, and our ongoing study is one of many that are seeking to answer these questions at the molecular and genetic level. But the evidence that supplementing mammograms with other imaging modalities can increase the rate of early detection is substantial, and provides us with tools we can use right now to make a difference. [3,4] Despite this progress, there are still significant hurdles in changing the standard of care. A recent experience with my routine breast cancer screening highlighted the ongoing challenges. When I had asked to schedule an ultrasound with my screening mammogram, I was informed that it was not done this way – I could only get a mammogram. After my mammogram, I had to wait to receive my letter in the mail approximately one week later to be able to take any additional steps. The interpretation included a description of breast density and recommended to discuss any additional care with my physician.
When I called to schedule an ultrasound, I was told that since the radiologist did not recommend it in the report, I could not schedule it. I then had to speak with my primary care provider, educating her on dense breasts and why I needed an ultrasound. Luckily, she agreed to order one. While the radiology facility still questioned the order, eventually I was able to have this done. When the radiologist came in to discuss my results, she too was confused as to why I was having the ultrasound, and was not aware that this should be standard for women with dense breasts.
Fortunately all was fine, but had I not been a physician that was fully aware of this issue, I would very likely have had only a mammogram and walked away with a dangerously false sense of security. This experience highlighted for me how much still needed to be done more than 20 years after my first experience. Legislation is only part of the solution. Clinician education and public awareness are the keys to changing how the intention behind these laws gets translated into actual change in health care.
As I experienced, many clinicians are ill-informed about the nature of dense breasts, and options for adjunctive screening including ultrasound or MRI. This means that many of these reports end up being filed away with no further action being taken that could make a significant difference in early detection and saving lives.
EPILOGUE: CURRENT STANDARDS VS NEEDS
ACOG still officially does not recommend any further imaging for women with dense breasts on mammogram, despite the significant body of evidence suggesting that mammogram alone is insufficient and adjunctive imaging with ultrasound or MRI increases rate of early detection. [5] The U.S. Preventive Task Force [6] does not recommend routine adjunctive imaging for screening women with dense breasts. This leaves many healthcare practitioners, from ObGyns to other primary care providers, unprepared to discuss this with their patients or provide sound recommendations.
The American College of Radiologists, who also publishes the BIRADS standards for breast cancer screening, acknowledges awareness of breast density detection issues with mammography but stops short of recommending routine adjunctive imaging. Instead, they list ultrasound and MRI as “may be appropriate”. [7] We have enough evidence to know how to better serve women with dense breasts, and we can do better. Now we need to push for better education of all primary health care providers, including ObGyns, and continue to raise awareness for women around current knowledge and best practices.

2024 CLINICAL PROFILE OF THE DENSE BREAST PARADIGM - for the Obstetrics & Gynecology Society
Published by ICRS Medical Press Ltd.
Breast cancer affects the lives of hundreds of thousands of women every year and is a leading cause of death. While we have made great progress in advancing earlier diagnosis and more individualized treatments, we still need to improve our approach to achieve our ultimate goal - prevention. This requires a deeper understanding of the molecular mechanisms and the multitude of factors that contribute to the development of breast cancer.
Dr. Roberta Kline, recognized speaker and publishing crusader for women's health brings you a comprehensive review and a deep-dive analysis of the current research findings about breast density and its major risk factors for breast cancer. Her reports uncover current imaging practices and clinical protocols updated in great support of breast density detection and the means of addressing this growing condition that affects over 45% of the female population. "Knowing a woman has greater breast density is a critical first step, but it doesn’t end there... we need to go further by understanding the causes of breast density, and how they relate to breast cancer-- we now have another avenue to proactively intervene to reduce risk or even prevent breast cancer in the first place." This textbook is a champion in targeting the
Dense Breast Paradigm as a blueprint and a clear course study for all clinical professionals who are dedicated to women's early detection and prevention programs.
(More information)WHAT ABOUT IF YOU'RE TOO YOUNG FOR A MAMMOGRAM? I went to my doctor for a lump I felt in my breast and she gave me a response that se...
FOR IMMEDIATE RELEASE NATIONAL CANCER ADVOCACY GROUP RECOGNIZES BARD DIAGNOSTIC RESEARCH FOR ADVANCEMENTS IN DENSE BREAST IMAGING 8/28/202...
1/19-2023- The ARE YOU DENSE ADVOCACY committee continued to pursue the public importance of patients receiving their own personal medical i...
References
1) Gordon PB. The Impact of Dense Breasts on the Stage of Breast Cancer at Diagnosis: A Review and Options for Supplemental Screening. Curr Oncol. 2022 May 17;29(5):3595-3636.
2) Chiu, S.Y.H.; Duffy, S.; Yen, A.M.F.; Tabár, L.; Smith, R.A.; Chen, H.H. Effect of baseline breast density on breast cancer incidence, stage, mortality, and screening parameters: 25-Year follow-up of a Swedish mammographic screening. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1219–1228
3) Harada-Shoji N, Suzuki A, Ishida T, Zheng YF, Narikawa-Shiono Y, Sato-Tadano A, Ohta R, Ohuchi N. Evaluation of Adjunctive Ultrasonography for Breast Cancer Detection Among Women Aged 40-49 Years With Varying Breast Density Undergoing Screening Mammography: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2021 Aug 2;4(8):e2121505
4) Mann, R.M., Athanasiou, A., Baltzer, P.A.T. et al. Breast cancer screening in women with extremely dense breasts recommendations of the European Society of Breast Imaging (EUSOBI). Eur Radiol 32, 4036–4045 (2022).
5) Management of Women With Dense Breasts Diagnosed by Mammography. ACOG Committee Opinion. CO Number 625 March 2015
6) https://uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-screening
7) American College of Radiology ACR Appropriateness Criteria® Supplemental Breast Cancer Screening Based on Breast Density. 2021
Copyright Notice: The materials provided on this website/web-based article are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and The AngioFoundation). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.








.jpg)

 EPILOGUE: CURRENT STANDARDS VS NEEDS
EPILOGUE: CURRENT STANDARDS VS NEEDS

 WHAT ABOUT IF YOU'RE TOO YOUNG FOR A MAMMOGRAM? I went to my doctor for a lump I felt in my breast and she gave me a response that se...
WHAT ABOUT IF YOU'RE TOO YOUNG FOR A MAMMOGRAM? I went to my doctor for a lump I felt in my breast and she gave me a response that se... FOR IMMEDIATE RELEASE NATIONAL CANCER ADVOCACY GROUP RECOGNIZES BARD DIAGNOSTIC RESEARCH FOR ADVANCEMENTS IN DENSE BREAST IMAGING 8/28/202...
FOR IMMEDIATE RELEASE NATIONAL CANCER ADVOCACY GROUP RECOGNIZES BARD DIAGNOSTIC RESEARCH FOR ADVANCEMENTS IN DENSE BREAST IMAGING 8/28/202... 1/19-2023- The ARE YOU DENSE ADVOCACY committee continued to pursue the public importance of patients receiving their own personal medical i...
1/19-2023- The ARE YOU DENSE ADVOCACY committee continued to pursue the public importance of patients receiving their own personal medical i...

