REMOTE IMAGING INTERPRETATION FROM THE DIAGNOSTIC INVESTIGATOR
By: Dr. Robert L. Bard

Dr. Cutter approached this project as more of a SURVEY, collecting data in various underserved communities- seeking out breast density in low BMI subjects as well as specific cultural groups. Her objectives aim to detect breast cancers in women under 39, or women with dense breasts that may not (yet) have the means or the capacity to access routine mammography or even clinical palpation by a physician.
*** See Dr. Noelle Cutter's Overview on this Phase 1 Study of Dense Breast Survey
SCANNER OF CHOICE: THE TERASON 3200t uSmart Portable Ultrasound
Upon review of a wide range of portable ultrasound devices, we selected the Terason 3200t (hereinafter shall be referred to as the Terason) due to its proven quality, user-friendly interface and its rugged design. Its capacity offers high resolution imaging and high quality probes that can capture anatomical scans comparable to hospital grade appliances. Hence, we are able to see not only the breast tissue, but also the skin. This means that if there's a breast cancer that's infiltrating the skin from below (which a clinician may not be able to see and oftentimes cannot feel) this will show that the cancer is a stage two because it's already broken through the bottom layer of the skin.
HUMAN RE-INTERVENTION IN IMAGING
While everybody's talking about artificial intelligence, the cancer imaging society continues to rely on seasoned experience of a seasoned diagnostic over-reader. Specifically, if there's a benign tumor that's calcified, it has the same look and effect as a breast cancer that's not calcified because calcium and cancer absorbs the ultrasound frequency the same way- whereby the area behind them is basically black, not white. So it takes an experienced eye to determine if something suspicious is really serious. As of now, artificial intelligence has not yet reached that level of sophistication in detective work.
WIFI SUPPORTS THE MEDICAL COLLABORATION PARADIGM
Today’s entire emergency response system is well underway the use of WIFI connected devices in their emergency vehicles. The portable rescue services are completely reliant on WIFI connections, allowing for field responders to receive medical guidance and diagnostic reading support from ‘central command’. Having access of the supervision of a senior medical professional on the field can save lives where precious seconds count- way before the patient arrives in the emergency room. The ability to have wifi allows the responder and the surgical team to confirm the pathology while receiving expert guidance from anywhere in the world within seconds.

PATIENT 1: STUDY OF BREAST LAYERS
This scan (Patent #1) shows that directly under the white line (A) is a black area that is the epidermis of the skin. The horizontal white band below is the dermis. The resolution of the Terason ultrasound device allows us to see less than half millimeter lesions. Below this is an area (B) that's mixed white and dark. It's got horizontal bands of white and broad swaths of dark fatty tissue, white is breast tissue. The scan shows normal breast tissue, which is gray.

To contrast from patient 1, we have band of white tissue (C), which is normal fatty breast tissue- appearing as white. Below C is the semi-circular bands represent the rib cage and more importantly, the surface of the lung. This is useful because should a cancer of the breast metastasize to the lymph nodes or to the lungs, this is where we might see evidence of this during this simple screening examination. The dense breast tissue is the band of white above the semi-circular rib cage echoes. And in the middle of the band of whites, you could see tiny black wormy lines, which represent dilated ducts, which are a part of breast disease or cystic breast disease.

Once again, the skin outline (Epidermal) is on the top, which the curvilinear ribs in the middle of the scan, which is a broad white path. And within the middle of this white path are tiny, bright white areas representing micro calcium inside the breast. The fibrous tissue is an inflammatory process which heals with scarring and calcification, which can also block the ducts and dilate the ducts. So here we have an example of a very white dense breast with areas of micro calcification, which are part of the healing process. This would be a CATEGORY 4 breast density on mammography because the tissue is homogeneously white.

PATIENT 7: BENIGN TUMOR
Here's an example of a benign tumor within the breast. Right below the word, right below the B. You have a black area within the white carpet of tissue, and it is sharply demarcated. It has echoes behind it. That is, there's a, a white trail behind the black area showing that it's a degenerated cystic area or a solid benign tumor that's breaking down into cystic regions. So this is an area that we follow, uh, every six months with ultrasound scans. This would show up as a BI-RADS or as a class four density and probably be missed on mammograms. In a prior research project, we did a study showing that the benign tumors like this in dense breasts are missed about 90% of the time by mammography. And of course, since the breast tissue is lumpy, they're often hard to palpate clinically.

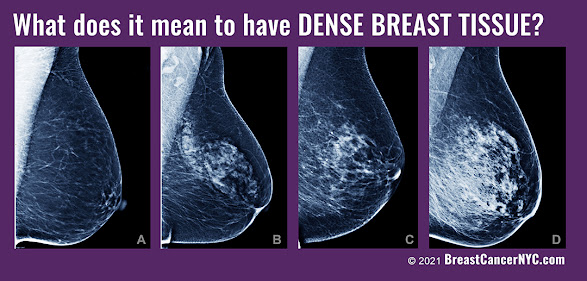
This is an example of a one density mammogram or breast tissue, because this is almost uniformly dark or fatty tissue within the breast. The linear white lines are prominent because the bulk of the tissue is predominantly fatty

This is an example of a class three. Here, we can see the white tissue interrupted by horizontal areas of dark and white indicating dilated ducts, some of which have micro calcification within them. Once again, we see the chest wall below that. So if there is a cancer, we can see if it's invading not only the skin, but the muscle tissue below that. With this technology, we can find cancers and stage them within minutes.

This is another example of mixed density tissue because you have alternating bands of gray and darker gray. Below that is a very thick pectoral muscle below, which is the white band of the rib cage. So we can see muscle disease as well as the pleural disease (on the lining of the lung). We can also measure the thickness of a muscle. This may be useful in treating muscle wasting diseases.

Breast density is a key factor in early detection because mammograms routinely miss breast cancer in dense breasts, especially in younger and more athletic women. Ultrasound offers a supplemental scan and peace of mind because it finds the pathology and almost instantaneously distinguishes from a benign cyst from a possible cancer - or a definite cancer. Ultrasound even goes further because if there is a definite cancer or something highly suspicious of a cancer, you can look at the other organs such as the glands under the arm to see if it's spread into the lining of the lungs to see if it's invading the pleura or the lymph nodes in the abdomen or the brain. Since we are now armed with expert diagnostic over-readers and remote collaborative imaging options, I urge our gynecologic and obstetric community to take advantage of this affordable non-invasive screening solution.